
Written by Jan Winhall
The Felt Sense Polyvagal Model TM (FSPM) is a healing paradigm that integrates Porges’ Polyvagal Theory, and Gendlin’s felt sense. While the model can be applied to any aspect of wellbeing, this paper focuses on the field of trauma/addiction. The two embodied processes of neuroception and interoception form the foundation of the model. Resting on that foundation are five theories that build the conceptual framework: 1) feminist trauma-informed theory; 2) focusing-oriented therapy/the felt sense; 3) interpersonal neurobiology; 4) learning model of addiction; and 5) Polyvagal Theory.
1. The Roots of the FSPM – A Feminist/Trauma Theory Framework
Over forty years ago, I began practicing as a somatic trauma therapist. My first job was leading groups for young women who were survivors of incest. I started reading feminist therapists, such as Judith Herman’s Trauma and Recovery (Herman, 1992) and Sandra Butler’s Conspiracy of Silence (Butler, 1978). They helped me to validate what I knew intuitively, that the top-down pathologizing model I was surrounded by was harming my clients. Feminist therapists understood how trauma and addiction happen in the body, and that we must help our clients to reclaim their embodied knowing. It was common knowledge in the feminist community that addictions were very effective and adaptive ways to attempt to regulate numbing and flooding responses. While many of us didn’t connect these responses to the autonomic nervous system (ANS), we honored the protective quality of addictions in attempting to regulate these polarizing states. Herman saw the connection.
“Abused children generally discover at some point in their development that they can produce major, though temporary, alterations in their affective state by voluntarily inducing autonomic crisis or extreme autonomic arousal. Purging and vomiting, compulsive sexual behavior, compulsive risk taking or exposure to danger, and the use of psychoactive drugs become the vehicles by which abused children attempt to regulate their internal emotional states. Through these devices, abused children attempt to obliterate their chronic dysphoria and to simulate, however briefly, an internal state of well-being and comfort that cannot otherwise be achieved” (Herman 1992, p. 109).
Herman explains the power of autonomic state-shifting that sometimes brings comfort and protection. This self-soothing behavior becomes addictive as it shifts the body into a numb and dissociated state of relief, and/ or a sympathetic surge of activation. We see this clearly in the binging and purging cycles that occur with dysregulated eating. Herman understood the function of addictions in the context of trauma as state regulation strategies. She described a continuum from intrusion, the sympathetic response, to constriction, the freeze response. She included the calm, dissociated state as part of constriction in the body. Back then, our understanding of dissociation was limited by the traditional model of the ANS. We now understand this “calm” state as descriptive of the collapsed, shutdown dorsal state that Porges integrated into the new understanding of the ANS. Porges’ contribution matched our clinical observations, and provided us with the missing piece. The state of collapse that appears to follow constriction explains the calm relief that our clients feel with profound dissociation and sleep. This is the place of relief that the body seeks when other forms of safety and comfort are unavailable.
Van der Kolk was curious about self-harming behavior (Van der Kolk, 2014). He asked, “Why are so many people attracted to dangerous or painful situations?” He conducted research with eight war veterans, who agreed to watch violent scenes from the movie Platoon (1986) while they took a standard pain test. They measured the length of time the veterans could keep their hands submerged in a bucket of ice water. They were then exposed to calm and peaceful scenes. They found that seven of the eight veterans kept their hands submerged in cold water thirty percent longer during the violent scenes. Van der Kolk states, “We then calculated that the amount of analgesia produced by watching fifteen minutes of a combat movie was equivalent to that produced by being injected with eight milligrams of morphine, about the same dose a person would receive in an emergency room for crushing chest pain”. (Van der Kolk, 2014, p. 33)
This research was profound in helping us make sense of our clients’ often-misinterpreted self-harming and addictive behaviors. Instead of assuming masochistic or attention-seeking explanations, we appreciate the role of the autonomic nervous system in shifting states to survive. We see how our clients re-enact their trauma stories by unconsciously returning to threatening situations that activate the release of endogenous opioids, creating a shift into a dorsal state of shutdown, and the calm relief that Herman spoke about.
Herman and Van der Kolk’s work in unravelling the mysteries of self-harm and addiction are wonderful examples of the integration of top-down and bottom-up approaches.
They listened to survivors with curiosity and compassion. By conducting qualitative and quantitative research, they contributed to unravelling the mysteries of the body and mind as they seek to survive unrelenting pain.
Feminist therapists also understood that establishing moment by moment safety was the most important part of the healing journey. I learned that creating a “safe nest” for our clients is essential for healing to begin. Safety is our North Star; it invites us, igniting a path and keeping us company as it points the way to connection. Without it, we are lost. Herman provided a three-stage model that created a safe container for the healing journey: establishing safety, remembering and mourning, and reconnection (Herman, 1992). Her work guided feminist therapists to create more structure and containment at the beginning of treatment, particularly in group therapy with survivors of sexual abuse.
Herman’s anti-oppressive lens provided a framework in which to understand the systemic nature of abuse on a personal and political level. This broad view of societal trauma provided a deeper, more sophisticated understanding of the challenges in creating safety for our clients, and in society.
2. Gendlin’s Focusing and Felt Sense
In developing the FSPMTM, I searched for a therapy that would help my clients reclaim their connection to body wisdom. In the mid-1980s, I found Gendlin’s book Focusing (1978). His contribution to the FSPMTM is found in the breadth and depth of his teachings. His philosophy of the implicit (Gendlin, 1997) offers a fresh way of integrating science and first-person experiencing. It teaches us that the body’s implicit knowing is beyond our conscious awareness. Gendlin discovered that clients who did well in therapy were connected to their body and its implicit knowing through what he called the felt sense. This knowing is at first vague. Turning attention inwards and noticing feelings and body sensations allows a felt sense, a whole sense of a situation, to form in the body. The felt shift arises as the body makes meaning from the felt sense. Embodied knowing is implied in the next step towards growth. Gendlin called this deep listening process Focusing. While it is a natural process, many people find it hard to do at first, perhaps because we live in such a disembodied culture. He made six steps to teach it to people.
Gendlin created the Experiencing Scale, (EXP;1986) that provides clinicians with a validated seven-point scale to assess the level of emotional and cognitive awareness of one’s ongoing experience. This interoceptive tool aids clinicians in tracking clients’ ongoing progress in deepening their capacity to integrate traumatic experience and strengthen their ventral presence. It is an essential part of the FSPM.TM
Gendlin encouraged the creation of Focusing partnerships. He believed that people were more often able to go deeper in their practice if they were accompanied by another person. Focusing is very much about listening to your partner in a way that honors their deep process. In this way, he created a powerful partnership practice based on the polyvagal concept of co-regulation. We help each other to connect and settle in our ANS as we deepen our Focusing practice.
Thoughts, feelings, physical sensations, and memories are avenues into the felt sense. In asking questions about these avenues, we help clients deepen their embodied knowing of an issue. As the felt sense forms, we pause and stay with the fullness of experiencing. Sometimes a felt shift, a physical release, happens as the client integrates new knowing. This relieving shift is the body’s way of pointing us in the direction of safety and healing. These shifts are what Gendlin called “the motor of change” (Gendlin, 1964) that carries us forward in life.
As I learned about felt shifts, it helped me to understand what I was observing in my clients’ bodies. As we worked through the trauma, I could see the physical shifts as their bodies opened and they became more present and socially engaged. With this presence comes a sense of meaning and purpose in life. This is vitally important, because trauma and addiction diminish and often shatter one’s sense of meaning and purpose.
When I began to read about Polyvagal Theory, I could see the interconnection between the subjective experience of a felt shift and the neurophysiological shift in autonomic states. My FSPMTM incorporated this theory, and posits that these felt shifts are, in fact, shifts in our autonomic nervous system that Gendlin would say “carry us forward.” This forward direction can be characterized as Porges’ ventral state of health, growth, and restoration.
3. Interpersonal Neurobiology
Dan Siegel’s work in helping us to understand the nature of mind-body interaction forms another layer of the FSPMTM. Siegel takes us into the world of interpersonal neurobiology (IPNB), an integration of subjective experiencing and traditional science. He deconstructs the pathologizing paradigm, creating a new way of understanding mental health. His model emphasizes the regulation of emotional states on a continuum from hyper-aroused to hypo-aroused. This work compliments Polyvagal Theory. Siegel understands wellbeing as a state of integration where clients learn how to regulate through mindfulness practices.
4. Lewis Learning Model of Addiction
In developing the FSPMTM I incorporated Marc Lewis’ (Lewis, 2015) learning model of addiction. The disease model argues that addiction changes brain chemistry. Lewis points out that brain changes, a process called neuroplasticity, that occur in addiction are the same as those that happen when we are in love, or absorbed in a sport. Thus, addiction is not a chronic disease, but a learned response – one that becomes habituated over time. This habituated response can also change as new neural exercises are learned, offering the addicted person hope in achieving a stable and healthy life. This de-pathologizing model of addiction provides a vital part of the FSPMTM.
5. Polyvagal Theory
When I discovered Polyvagal Theory, I knew I had found the missing piece for my evolving model. I was now able to clearly see the functional role of addiction as activating a blended state of both the sympathetic and dorsal branches of the ANS. The theory resonated with me in three powerful ways: 1) Porges’ emphasis on safety as the precursor for healing; 2) his identification of both the dorsal branch of the ANS and the social engagement system; 3) the concept of autonomic state as the intervening variable in the traditional stimulus-response model.
Safety as the Precursor of Healing
Understanding addiction within the context of both an absence of and a quest for safety is a powerful framework. It challenges us to examine our understanding of what constitutes safety, and how lack of experiences of safety relate to trauma and the prevalence of addictive behaviors. Indeed, the research that links trauma and addiction is impressive, as emphasized by Porges, above (e.g. Carliner, Keyes, McLaughlin, Meyers, Dunn & Martins, 2016; Enoch, 2011; Felitti, 2006).
So, what is safety? The answer to this question differs greatly depending on what framework you employ. Our culture’s current top-down approach typically understands safety as the absence of physical threat (Porges, 2017). We concentrate on making environments safe by building walls, fences, security systems, and jails. Our actions are driven by fear. We often fail to address our very real need to actively create cues of safety. When our needs for “enough safety” are not met, we are often traumatized by a culture that blames individuals instead of examining societal systems of oppression. Many of our clients live in chronic states of dysregulation, having learned to deal with traumatizing conditions by using substances and behaviors to alleviate overwhelming feelings of isolation. In terms of addiction, we create a “war on drugs,” and then criminalize those suffering from addiction. In our current dissociated state, we fail to see the systemic causes of trauma and addiction.
From a bottom-up perspective, we view safety quite differently. While physical safety is important, it remains one dimension of our experience. Porges notes that feeling safe is akin to a felt sense. When we tap into our felt sense of safety, we become aware of thoughts, feelings, physical sensations, and memories. We have an embodied sense of connection with our emotional and physical needs. When we are connected to embodied knowing, we realize the importance of creating safe spaces that address all our needs: physical, emotional, sensory. When we nourish these parts of ourselves, we become interconnected as a species. We appreciate the inequalities that exist in our world, and how those inequalities create trauma and addiction. And, we understand the importance of repair instead of punishment.
From a polyvagal perspective, we must consider not only our clients’ need for safety, but also our own. We understand that we co-regulate each other’s ANS, and therefore need to create the conditions upon which we will both feel safe enough to grow together.
Unfortunately, our professional boundaries reflect the top-down methodologies that are currently dominating our therapeutic work. Forty years ago, the field of trauma was very underdeveloped. As we began to address issues of abuse and neglect, we were told that we should stop asking clients if they were abused, for fear of implanting “false memories” (Loftus, 1996). We were instructed not to touch our clients, as that could trigger them. We were told that they couldn’t distinguish between safe touch and sexually abusive touch. Many of us were afraid of being sued or sanctioned by our colleges, and an appalling sense of fear silenced us. I would argue that this fear is still shaping our professional standards. As therapists, we must feel safe enough to foster a warm, deeply intimate space in which to hold our clients. We must have the courage to move beyond fear, and share our own authentic self. When we share our own vulnerability in a carefully bounded way, we model what it is to be human in all its rich and various forms. As humans, wired to connect, we need to feel free to acknowledge our enjoyment of each other, and to relax into being ourselves. After all, we are engaging with our clients in an arduous and lengthy journey. Our commitment is fed by our enjoyment of the relationship.
Our job as therapists is like no other. We need to be able to create moment by moment experiences of enough safety so that healing can begin. From a polyvagal perspective, this requires much from us. We are our own instruments in the work. We cultivate, as much as possible, a grounded awareness and embodied connection with our clients. We do not have to be fully grounded, but we do need to be grounded. We gently and steadfastly coax the person we are accompanying into “eyes wide open” presence. This is facilitated by much patience, and often love, for our clients. It requires us to be firm in holding them accountable when facing the truth about their lives. As we build the safe nest, they will lean into us. We have to stand tall, like the oak tree. It bends in the wind, but it must stay standing.
Identification of the Dorsal Vagus and Social Engagement System
Porges’ identification of the unique functions of the dorsal branch of the vagus nerve as part of the ANS facilitated a huge shift in the trauma world. It provided a clear understanding of the powerful numbing and shutting down experiences that we see in our clients’ responses. We now appreciate the immobilizing effect of the dorsal state when the body is under great threat. Polyvagal Theory provides a top-down and bottom-up theory that explains the full range of options in the ANS, from sympathetic to dorsal responses. The shutdown, numbing function of the ANS can now clearly be identified as separate from the commonly called freeze state.
The freeze state is now understood as a blending of sympathetic mobilization and dorsal immobilization, resulting in a stuck process in the ANS. The body constricts with the sympathetic surge, but it is simultaneously immobilized with dorsal activation, creating a stopped process. This identification of the freeze state leads us to a deeper understanding of the role of addictions as state regulation strategies in the ANS. This stuck process is a powerful feature of addiction. From a polyvagal perspective, it makes sense that addictions act as propellers that shift the body along this continuum in a quest for safety. Sadly, as Porges points out, even if these behaviors bring temporary relief, they create an endless feedback loop that results in unsuccessful attempts to regulate.
Norman Doidge describes this state as the “plastic paradox” (Doidge, 2017). The process of neuroplasticity – the way in which our brains are always changing – paves the way for healing from trauma and addiction. However herein lies the paradox: if behavior is repeated too often, as in addiction, the neural pathways become rigid and unchanging. Then, the addicted person is literally in a rut – spinning their wheels and going nowhere.
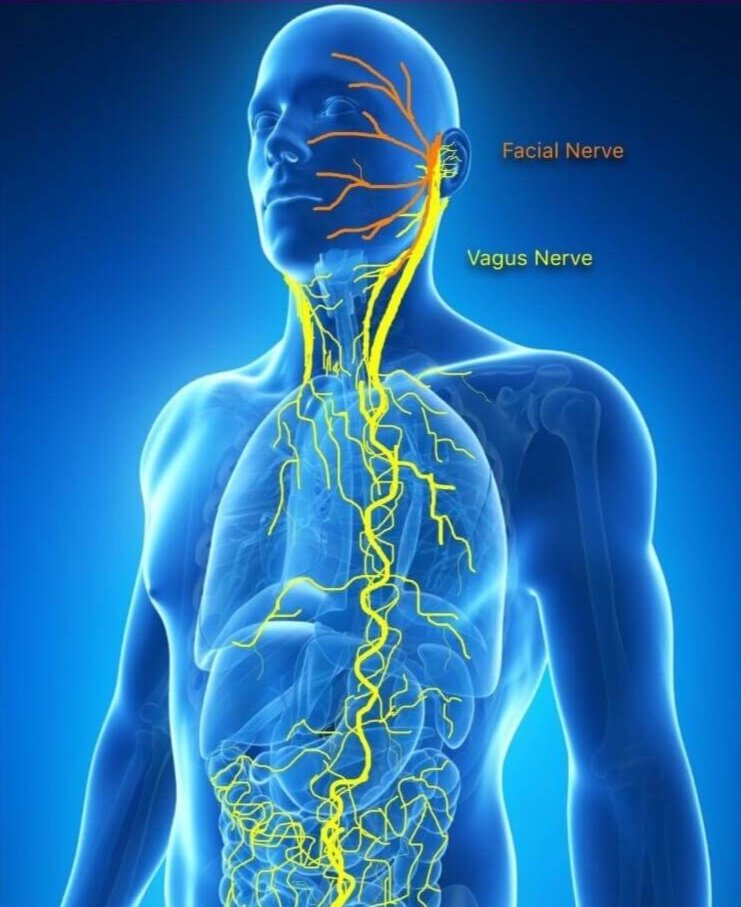
The social engagement system is a term coined by Porges that describes the cluster of neural pathways that interact in the ventral vagal complex to support sociality, while simultaneously supporting health, growth, and restoration (Porges, 1998). The ventral vagal complex is a brainstem area that regulates the ventral vagal pathways and the striated muscles of the head and face. The ventral vagus communicates with organs above the diaphragm, and facilitates bidirectional neural communication between the face and the heart. This demonstrates how we are wired to connect through our facial expressions and prosody of voice.
The social engagement system is activated when we feel safe enough to be grounded and present. We have the capacity to connect with others, and think through how we want to respond to situations, especially those that require empathy and good judgment. When we lose this connection due to activation of defensive states, our capacity to think clearly and respond with empathy is debilitated. In the state of addiction, the ventral vagal complex is compromised. We lose our clear-headed and compassionate selves. This is how good people can find themselves doing bad things. People who are addicted are compelled by a neurophysiological drive to acquire whatever it takes to self-soothe. The body is wired to survive, and in a desperate state the social engagement system is severely compromised.
This understanding is key to revolutionizing addiction treatment. Rather than invoking addictive metaphors of devils or greedy monsters that must be defeated, we describe the process in our autonomic nervous system that shifts the body into states of defense to survive. In chronic defensive states – the addictive loop – we lose our capacity to think clearly. Illegal and immoral acts then become options in our repertoire of behaviors. Appreciating the body’s attempt to keep us alive enables us to befriend the body, rather than treating it as a war zone. In my experience, explaining this to clients is life-changing. It creates what I call “moments of liberation” from endless shame and despair. It sheds light on the profound confusion that clients have in understanding how they could have behaved in ways that they often abhor. These moments are the treatment! This understanding brings powerful felt shifts into ventral states of repair as clients learn to hold their addicted parts with love and kindness.
Knowing that our clients will want to avoid social engagement helps us to understand why the treatment of choice, group therapy, will be a scary proposition for most. I start with individual sessions, building co-regulation over time. As we establish some safety and connection, most clients will take a risk with group, especially knowing that I will be there to lead.
Autonomic State as Intervening Variable
Polyvagal Theory suggests that our autonomic state determines how we will experience the world. Our ANS is the intervening variable in the traditional stimulus-response model. Simply put, when we are stimulated by an experience, our present autonomic state will determine our response. I will give an example.
As I write this today, large numbers of people are demonstrating against vaccine mandates and other Covid measures in a movement for “freedom.” They are gathering in mounting numbers by foot, and driving large trucks into the center of the city. As they approach, a few miles from my home, they are chanting and honking horns incessantly. I listen to the news, and hear about police presence, and the concern that these trucks will attempt to block access to hospitals. I sense the momentum building, and feel a surge of sympathetic energy flow through my body. I am moving into a state of defense.
As I respond from this sympathetic state, I feel scared and angry. My body is mobilizing, and I want to hide or fight back. I feel judgment and despair about this behavior. If I invite my body to settle and engage in ventral energy, a felt sense of enough safety forms in my body. The story that follows from this ventral state is different. I understand that these folks are upset, and perhaps feel helpless and frightened by the very prolonged Covid measures that they are enduring. They too are surging into sympathetic flight/fight responses without much ventral capacity.
I understand that in order to move into social engagement and co-regulation, our officials will have to facilitate a way forward by listening to each other. As I breathe and stabilize, I feel much less judgment and much more capacity to empathize.

Anti-Oppressive Theory
The FSPMTM is held by and accountable to anti-oppressive theory. From this lens, we understand the root causes of addiction and their role in the autonomic nervous system. Our culturally condoned systems of oppression lead to trauma, and trauma is the underbelly of addiction. Consequently, marginalized groups are much more vulnerable. Staci Haines, author of The Politics of Trauma (2019), puts it so well when she says that trauma robs us of safety, belonging, and dignity. Without these basic needs being met, we seek out twisted ways of soothing to help us survive.
Introduction of the Graphic Model Clinician and Client Versions
The graphic models help clients become familiar with the ANS using imagery. By visualizing images, we engage a bottom-up process that helps clients embody the concepts and pathways to healing through activating the right hemisphere. The use of these models early on in treatment accelerates the ability to befriend the body by harnessing the ANS and the felt sense as powerful vehicles for change.
To support the FSPMTM, I created two graphic models 1 – one for clinicians and one for clients. My clients helped me create a simple version where each state starts with the letter F to make it easy to re- member. They keep track of their state by putting a picture of the model on their phone and/or their refrigerator. We call it orienting to the Six F’s when we discuss the model. Together, we track states, tracing the pathways, as a way of describing the healing journey. The graphic images help clients see very clearly how addictions function as propellers between flight/ fight and fold. The top half of the model shows the trauma pathways where the ventral social engage- ment system is compromised. The bottom half fol- lows the ventral pathways, the states that support a fulfilling life.
Applying the Felt Sense Polyvagal ModelTM Embodied Assessment and Treatment Tool (EATT)TM
When I began working with the FSPMTM I realized that I would need to create an assessment tool that captured the experiential process of the work and the somatic history of the client. The traditional bio-psycho-social assessment is completed in the first or second session. It focuses on taking a detailed assessment of the client’s history, with no reference to embodied processes. There are many problems with this approach. For example, clients are required to share detailed traumatic experiences and addictive behaviors all at once, and at the beginning of treatment, when a sense of safety is just beginning to be explored. At the very least, this is uncomfortable for clients, and at worst it is retraumatizing.
In sharp contrast, the Embodied Assessment and Treatment Tool (EATT)TM 2 slowly integrates assessment and treatment over time. In keeping with the experiential nature of our work, and the attention to body process, the client’s history unfolds as the body reveals its wounded places. By tracking neuroception (polyvagal theory) and interoception (focusing) as our framework, we develop a comprehensive assessment package that documents ongoing progress, and provides the client with therapeutic tools and practices they can use as resources in their healing journey.
The Importance of Asking
If your early assessment with a client indicates a lack of ventral presence for significant periods of time, it is important to consider that they may be using self-harming and potentially addictive substances and behaviors to manage neurophysiological state changes. It then becomes essential, from a polyvagal perspective, to explicitly ask about self-harm and addiction. We need to bring the body on board, to recruit the ANS as a collaborator in helping us unlock the addictive pathways, by shifting neuroception. When we work with the body, we invite all the parts of a person to embrace the idea of reducing harm. Otherwise, we engage in an unspoken power struggle: the mind wants to stop addiction, but the body is stuck in a ANS trauma loop.
With the FSPMTM as our guide, we begin to track the client’s autonomic state and capacity for embodied experiencing. The tool has eight components that include the following:
1. The Felt Sense Polyvagal ModelTM
2. TheExperiencingScale (EXP,1986)
3. The Felt Sense Polyvagal DialogueTM
4. TheThreeCircles (Carnes,2001)
5. TheTraumaEgg (Murray,2012)
6. The Nine Domains of Integration (Siegel, 2012b)
7. The Privilege Wheel, (https://www.oise.utoronto. ca/edactivism/Activist_Resources/The_Power_ Flower.html)
8. SpecificConcerns
In a top-down approach, we would use each of these in order. I start by tracking neuroception with the FSPMTM and interoception, using Gendlin’s Experiencing Scale. Then I use the rest when, and if, they become helpful in our experiential journey. For the sake of brevity in this article, I will give a case example using the FSPMTM and the Three Circles practice by Patrick Carnes. For a detailed description of the Felt Sense Polyvagal DialogueTM that I used in this case, see Chapters 13 and 14 in my book Treating Trauma and Addiction with the Felt Sense Polyvagal Model (Routledge, 2021).
A Case Example – Lily and Lucas
Lily, a hip young woman in her mid 30s, came to see me five years ago. She and her partner Lucas met at a ballroom dancing course. They fell into a routine of going for drinks after class. Over time, they moved in together, and the drinking became a nightly routine. It was never enough to prevent either of them from performing well at work, but Lily was feeling more and more uneasy about it.
During our time together Lily and I explored the feelings that surrounded this behavior. She learned how to connect with her felt sense of the problem. It came quite naturally to her, since she was a trained dancer. She became adept at understanding her calmed and smoothed the jagged edges of her anxious state. Together we traced the addictive pathways from Fight/ Flight (sympathetic) to Fold (dorsal) with alcohol and sugar planted firmly in Fixate(sympathetic/dorsal). She resonated with the understanding of addictions as propellers that shifted her from one extreme to the other. She appreciated how the addictive neural pathways were in the top half of the FSPMTM, limiting her capacity for social engagement and a feeling of safety. We used Carnes’ Three Circle Practice to help Lily make a harm reduction plan and be accountable to herself. This practice, called a neural exercise in polyvagal language, helped Lily create new ways of finding grounding energy that moved her into Flock, Flow, Fun (ventral).
Body Cards
In keeping with the enhancement of bottom-up processes in working with the FSPMTM, we use Body Cards to invite the client to draw the felt sense of a neurophysiological state. The imagery helps to explicate the implicit experience, and in the case of ventral states, the cards can be used as resources. Here is an example of a Fight/Flight sympathetic state Body Card.
The Three Circles
The Three Circle practice is a tool that was developed by Patrick Carnes (2001) in his work with sex addiction. The three concentric circles provide a map for clients to document their management of addictive behaviors. I integrated the ANS states into the three circles.
The Inner Circle: Fixate
The inner circle represents addictive behaviors that clients are ready to change. We work with the process by using the FSPMTM as our guide.
By explaining the model, we are recruiting the person’s nervous system to collaborate in the healing process. We invite the body to consider letting go of addictive behaviors. When clients are ready, we place the behaviors inside the circle. The behaviors must be quantifiable for clear accountability. Clients agree to check in with their therapist to build accountability on a daily or weekly basis, and/or they can check in with their focusing partner. If they want to change the boundaries around the behaviors, they agree to negotiate with their therapist first.
Lily’s inner circle contains no alcohol, and two desserts per week.
The Middle Circle: Fight/Flight, Fixate/Freeze, Fold
The middle circle represents the stressors, the experiences that lead to the activation of the addictive behaviors. These can be current-day stresses like job problems, conflicts in relationships, systems of oppression, poverty, and early abuse histories. We trace the ANS states on the FSPMTM to help clients begin to understand how these soothing behaviors ease anxiety and rage. They begin to appreciate how addictions act as state regulation strategies, propelling them often from flight/fight to fixate to fold. They appreciate the adaptive nature of their very bad habits when flock was not available.
Lily’s middle circle contains stress at work, loneliness, anxiety, and feelings of shame that are profound and confusing.
The Outer Circle: Flock, Fun/Fired Up, Flow
The outer circle is the sweet spot where bodies feel safe enough to engage in social interaction, to rest, to digest, to trust. It is the place of health, growth, and restoration in the body. The felt sense experience of life is engaged, and purpose and meaning carry us forward in a productive life. Addictions are not active in this state of social engagement.
Lily’s outer circle contains:
- ◼ doing daily practices including checking Three Circles and FSPMTM
- ◼ spending time with friends and family, and with Lucas
- ◼ teaching dance, yoga
- ◼ attending weekly therapy sessions
- ◼ Focusing weekly with her partner
Lucas Joins Us
Lily was making some progress with the use of the Three Circles and the FSPMTM, but she was finding it difficult without Lucas’ participation. When we invited him to join us, he was eager to begin his own journey. Lucas did his Three Circle Practice so they could work together on a plan. They both agreed to stop drinking alcohol, placing “no alcohol” in the inner circle. They cultivated their outer circle behaviors, and their relationship began to settle into a flock, flow, and fun rhythm. We said goodbye for now, and I didn’t see them again until I got a call from Lily about a year later.
The Call
I opened my office door to tall, elegant Lily, dressed in gorgeous colors and delicate silver earrings. My body remembered beautiful, vulnerable Lily with a loving feeling of delight. But something was terribly wrong. Lily sat down and collapsed into our warm space. She had discovered that her handsome, safe, and loving Lucas, the man she trusted as kind and honest, was hooking up with men for sex.
As she shared this with me, Lily fell into a dorsal state of shock, her body folding into the couch, eyes sinking into oblivion. I felt alarmed, and leaned in. I whispered to the Lily that I know, coaxing her back to breath, back to me and to life. She began to surface, breathing more deeply as she returned to the room, but her eyes held mine with a despairing gaze. It was hard to greet her here, in such a painful, dark place. But that is our job, to be present and hold these places with love and care. This is the arduous work of co-regulation. I gently extended my hand, and she reached over, hungry for the anchoring warmth of touch. We paused and breathed, feeling our feet on the ground.
The Healing Journey
Lily, Lucas and I met over several years. Together, we explored their embodied stories through the relational felt sense, the body’s way of co-regulating. We started by building a safe nest together. They revisited the Three Circle Practice and Lucas agreed to add “no use of pornography” and “sexual activity only with Lily” to the inner circle. We checked in at the beginning of each weekly session to help them be accountable to each other as the therapy progressed. Over time more of their trauma stories were revealed as we moved deeper into the wounded places. This work is the heart of the journey, excavating the trauma that forms the underbelly of the addictive behaviors.
As Lucas connected with his felt sense, deepening his capacity for experiencing, he was able to share more of his struggle with obsessive use of pornography, and unsafe sexual encounters with men. He was confused and frightened by this behavior describing it as an ‘out of body, mechanical” feeling that came over him. It seemed clear that this behavior was addictive. He wanted to stop but was struggling to stay grounded.
As they established safe boundaries in their relationship, we worked through the trauma using the FSPMTM to help them understand their ANS pathways. They became familiar with their default autonomic states. Lucas was aware that he lived much of his life in a somewhat dorsal state – seeking aloneness and shutting down intense emotion. Lily recognized her general tendency towards sympathetic activation, often feeling the full range of fight/flight feelings. She acknowledged that she flew into raging at Lucas when she was angry, which activated his shutdown response. Lucas began to cry as he heard Lily’s acknowledgement of her anger. To hear her capacity to give to him now, after he had hurt her so deeply, was overwhelming for him. He was as confused by his acting out behavior as Lily was, but he knew his confusion was not an excuse. He was responsible for hurting her. I saw him slowly peek at Lily, as he tried to find his voice.
“It feels really good to hear you acknowledge your rage. When you yell, I die inside… In fact, right now my heart is racing.” Lily asks Lucas to check down into the center of his body and see what is happening now. “It feels shaky, like butterflies in my stomach. I can see that red ball, like the fight/flight place on the model, in my gut. It feels good though to talk openly with you, and for you to hear me.”
Lily mirrors back, and I see a moment of connection deepen between them for the first time since this all happened. Together, we pause and help Lucas explore more of his felt sense. He checks in with the butterflies in his stomach, the red ball in his gut. He shares that it feels calmer in there now, more relaxed, and expansive. I tell him that we call this the felt shift when the body changes neurophysiological states. “Like going from flight to flock,” he says.
“Yes!,” I say, and we all laugh (Winhall, p. 203).
From time to time they both slipped in their efforts to not drink alcohol. Lily did well with her two desserts a week. Lucas was able to stop hookups with men, but did occasionally slip into watching pornography when Lily was traveling for work. This caused a lot of re-experiencing of the trauma. I decided to refer Lucas to a Focusing-oriented sex addiction group for men, and Lily to a women’s group.
During their separate therapy sessions, Lily and Lucas both awakened early memories of sexual abuse. While these memories were never completely dissociated, they lay dormant in the body. As the body healed, more of the story emerged. They eventually revealed to each other, with heart-wrenching tenderness, their shared histories of child sexual abuse. Lily shared a history of being abused as a little girl by her uncle and his friend. Her body takes her back to the felt experience of the abuse, and her soothing with food. This connection is powerful, and creates a felt shift for Lily. Fragments of feelings and behaviors start to fall into a cohesive narrative about her life. Lucas and I can see the physical release in her body as she settles into a ventral state of relaxation.
Through his work in the group, Lucas began to make deep connections with past and present behaviors. He was able to share memories of being sexually abused by an older male neighbor, and a teacher. By tracking his felt sense of these memories, he began to connect his hookups with the same feelings that originated in these early experiences – a deeply confusing mixture of sexual excitement and repulsion. While he still wasn’t clear about it all, he was beginning to understand that his body was taking him back to wounded places that he needed to make sense of. He realized how the acting out was followed by a deep dorsal state of numbing, bringing him relief from anxiety and depression. Now it became clear to both of them how the abuse activated the middle circle dysregulated trigger states, subsequently leading to their inner circle addictive behaviors. They both recognized how their addictive behaviors told a deeper story about their lived experiences.
The couple still struggled in their relationship. While Lucas no longer identified as being sexually addicted, he challenged the relationship in his need to explore his sexual orientation. While unclear, he was very committed to Lily, not wanting to lose the deep intimacy they had created. Lily grew to accept that Lucas was attracted to many kinds of sexual expression, but for now she needed him to be monogamous. For now, he agreed.
Moments of Liberation and Couple Felt Shifts
“So, we have little Lily and little Lucas, child parts that learned about sexuality in a scary way. A way that was confusing and robbed them both of the right to decide how and when to share that part of themselves. As I say this, we all start to cry. I try to honour my tears and at the same time, tuck them inside so I can be here for this wonderful moment of liberation for Lily and Lucas. As we unravel the triggered places, I invite us all to notice the felt shifts as we sense into this exquisite moment” (Winhall, p. 210).
The Five R’s for Addiction Treatment
I have adapted Deb Dana’s four R’s as they apply to the Felt Sense Polyvagal ModelTM for addiction. They summarize Lily and Lucas’ healing journey. They are as follows:
- ◼ Reframe addictions as state regulation strategies
- ◼ Recognize and explore the autonomic state/felt sense
- ◼ Respect the adaptive survival response
- ◼ Regulate or co-regulate into a ventral vagal state
- ◼ Re-story [Adapted from Deb Dana] (Dana, 2018, p. 7)
Lily and Lucas were able to re-story the rupture in their relationship by working through their early abuse histories. The Felt Sense Polyvagal ModelTM helped them reframe their addictive behaviors and respect them as state regulation strategies that were adaptive survival responses. By recognizing and exploring their ANS and their relational felt sense, they were able to co-regulate into a ventral vagal state.
Conclusion
Polyvagal theory and the work of Stephen Porges makes a major contribution to our understanding of addictive behaviors. In the language of Polyvagal Theory, we understand that behaviors are emergent properties of a neural platform mediated by autonomic state. A behavior viewed as pathological in one setting can be adaptive in another setting. Addiction disrupts feelings of safety and sociality through changes in autonomic state that function as an intervening variable, biasing reactions to context. Although addiction strategies are an attempt to dampen underling feelings of threat, the strategies frequently downregulate the bidirectional feedback loops, resulting in a numbing process that may have short-term benefits in relation to physical pain and mental distress, but in the long term, dampened neural regulation of visceral organs may lead to end organ damage.
In the optimal social context of humans, social interactions serve as the prominent mechanism to calm the autonomic nervous system. In contrast, in the world of addiction, social interactions are displaced by drugs and behavior to regulate the autonomic nervous system, thus disrupting homeostatic functions and potentially compromising mental and physical health.
The Felt Sense Polyvagal ModelTM is grounded in Polyvagal Theory, and integrates the work of Eugene Gendlin’s Focusing Oriented Psychotherapy, as well as Marc Lewis’ learning model of addiction. It is a generic framework that provides an embodied, comprehensive, non-pathologizing model for understanding and treating trauma and addiction. The model brings addiction treatment into the world of somatics, and can provide the psychotherapist with a framework for any treatment modality that they are currently using.
This paper offers a new and deeply embodied way of understanding and treating addiction. Bringing attention to the body’s autonomic nervous system, our safety monitor, reveals the protective qualities of addiction when faced with prolonged feelings of isolation and lack of enough safety. By recruiting our nervous system as a collaborator in the healing process, we tap into the key to successful treatment, establishing safe enough spaces for healing to begin. We know that addiction is created and prolonged by states of vulnerability. Embodied psychotherapists see the trauma of addiction every day. We see how the addicted person is stigmatized. “The drug addict is today’s scapegoat,” says Gabor Maté (2008, p. 58).
It is easier to offer brain disease models than to address the source of the problem by dismantling systems of oppression that undermine safe spaces. But there is a growing social movement that seeks embodied approaches – a movement that longs for connection, cooperation, and dignity for all. While we may appear to have lost our way, it is only in our heads. Our bodies know the answer.
Keywords:Addiction, felt sense, polyvagal
About the authors:
Jan Winhall, M.S.W. F.O.T., is an author, teacher, and psychotherapist. She is an Adjunct lecturer in the Department of Social Work, University of Toronto. Jan is Director of Focusing on Borden, a psychotherapy and training center, and a Coordinator with the International Focusing Institute. She teaches internationally on trauma and addiction.
Stephen W. Porges, PhD, is a distinguished university scientist at Indiana University, where he is the founding director of the Traumatic Stress Research Consortium. He is professor of psychiatry at the University of North Carolina and professor emeritus at the University of Illinois at Chicago and the University of Maryland. He has published more than 400 peer-reviewed scientific papers. He is the creator of the Polyvagal Theory and a music-based intervention, the Safe and Sound ProtocolTM, currently used by more than 2000 therapists to reduce hearing sensitivities, improve language processing, and increase spontaneous social engagement. He is a co-founder of the Polyvagal Institute. He is the author of The Polyvagal Theory: Neurophysiological Foundations of Emotions, Attachment, Communication, and Self-Regulation, The Pocket Guide to the Polyvagal Theory: The Transformative Power of Feeling Safe, and Polyvagal Safety: Attachment, Communication, Self-Regulation, and co-editor of Clinical Applications of the Polyvagal Theory: The Emergence of Polyvagal-Informed Therapies.
REFERENCES
Butler, S. (1978). The Conspiracy of Silence: The trauma of incest. Volcano, CA: Volcano Press.
Carliner, H., Keyes, K. M., McLaughlin, K. A., Meyers, J. L., Dunn, E. C., & Martins, S. S. (2016). Childhood trauma and illicit drug use in adolescence: A population-based national comorbidity survey replication – adolescent supplement study. Journal of the American Academy of Child & Adolescent Psychiatry, 55(8), 701-708.
Carnes, (2001). Out of the shadows: Understanding sexual addiction (3rd ed.). Center City, MN: Hazelden Publishing.
Dana, D. (2018). The Polyvagal Theory in Therapy. New York: W. W. Norton & Co.
Doige, N. (2007). The brain that changes itself: Stories of personal triumph from the frontiers of brain science. New York: Viking.
Enoch, M. A. (2011). The role of early life stress as a predictor for alcohol and drug dependence. Psychopharmacology, 214(1), 17-31.
Felitti, V. J. (2006). The origins of addiction. Evidence from adverse childhood experiences. [https://nijc.org/pdfs/Subject%20 Matter%20Articles/Drugs%20and%20Alc/ACE%20Study%20-%20OriginsofAddiction.pdf]
Gendlin, E. T. (1964). Theory of personality change. In P. Worchel & D.Byrne (Eds), Personality change. New York: Wiley. Gendlin, E. T. (1978/1981). Focusing. New York: Bantam Dell.
Gendlin, E. T. Focusing oriented psychotherapy: A manual of the experiential method. New York: Guilford Press.
Gendlin, E. (2017). A process model. Evanston, IL: Northwestern University Press.
Gerge, A. (2020). What neuroscience and neurofeedback can teach psychotherapists in the field of complex trauma: Intero- ception, neuroception and the embodiment of unspeakable events in treatment of complex PTSD, dissociative disorders and childhood traumatization. European Journal of Trauma & Dissociation, 4(3), 100164.
Haines, S. (2019). The Politics of trauma. Berkeley, CA: North Atlantic Books. Herman, J. (1992). Trauma and recovery. New York: Basic Books.
Klein, M., Mathieu-Coghlan, P. L., Gendlin, E. T., & Keisler, D. (1970). The experiencing scale: A research and training manual
(Vol. 1). Madison, WI: Wisconsin Psychiatric Institute.
Lewis, M. (2015). The Biology of Desire: Why addiction is not a disease. New York: Public Affairs.
Loftus, Elizabeth (1996). The myth of repressed memory: false memories and allegations of sexual abuse. New York: St. Martin’s Press.
Maté, G. (2008). In the realm of hungry ghosts: Close encounters with addiction. Toronto, ON: Alfred A. Knopf Canada.
Murray, Marilyn (2012). The Murray method: Creating a wholeness beyond trauma, abuse, neglect and addiction. Vivo Publications.
Nov 30th 2017, ISNB-10 0985509317.
Porges, S. W. (1995). Orienting in a defensive world: Mammalian modifications of our evolutionary heritage. A polyvagal the-
ory. Psychophysiology, 32(4), 301-318.
Porges, S. W. (1998). Love and the evolution of the autonomic nervous system: The polyvagal theory of intimacy. Psychoneu- roendocrinology, 23, 837-861.
Porges, S. W. (2011). The polyvagal theory. New York: W.W. Norton & Co.
Porges, S. W (2017). The pocket guide to the polyvagal theory: The transformative power of feeling safe. New York: W.W. Norton & Co.
Porges, S. W. (2021). Polyvagal Theory: A biobehavioral journey to sociality. Comprehensive Psychoneuroendocrinology, 100069.
Siegel, D. J. (2021b). The developing mind, second edition: How relationships and the brain interact to shape who we are. New York: Guilford Press.
Van der Kolk (2014). The body keeps the score. New York: Penguin Books.
Winhall, J. (2021). Treating trauma and addiction with the felt sense polyvagal model bottom-up approach. New York: Routledge.
From International Body Psychotherapy Journal The Art and Science of Somatic Praxis
Volume 21, Number 1, Spring/Summer 2022, pp. 13-31
ISSN 2169-4745 Printing, ISSN 2168-1279 Online
© Author and USABP/EABP.
